A couple years ago, I worked with Mr. Davis, a Black man who was 85 and held a strong Jehovah’s Witness faith. He was in therapy due to a recent separation from his wife. This resulted in lowering his position in his Jehovah’s Witness congregation. New medical issues were cropping up and he was exploring “who will be there for me” in therapy.
To help me get to know him, Mr. Davis brought in Jehovah’s Witness pamphlets. I accepted them and asked Mr. Davis to tell me why these pamphlets were so important. I took the right steps but beneath the surface, I was skeptical of his faith and began projecting my negative experiences with fundamentalist Christianity onto him. In therapy, my bias resulted in my tendency to focus on conflicts Mr. Davis had with his faith, rather than the support and connection he gained from it.
I was a newly married White woman in my early 40s with a complex history of oppression by my fundamentalist Christian faith. I prided myself in providing culturally humble care and had been doing so for many years, but somehow, with Mr. Davis (a man for whom I cared deeply), I was failing. Focusing on the points of conflict in Mr. Davis’ faith community added turmoil that could cause Mr. Davis more harm as he was looking for a place of belonging, not reasons to leave. My desire to protect him could have easily created as a white savior dynamic and disempowered him when he was feeling particularly vulnerable. It took a practice of self-reflection, consultation, and humility to help me see how I might be unconsciously shaping therapy due to my own unconscious bias.
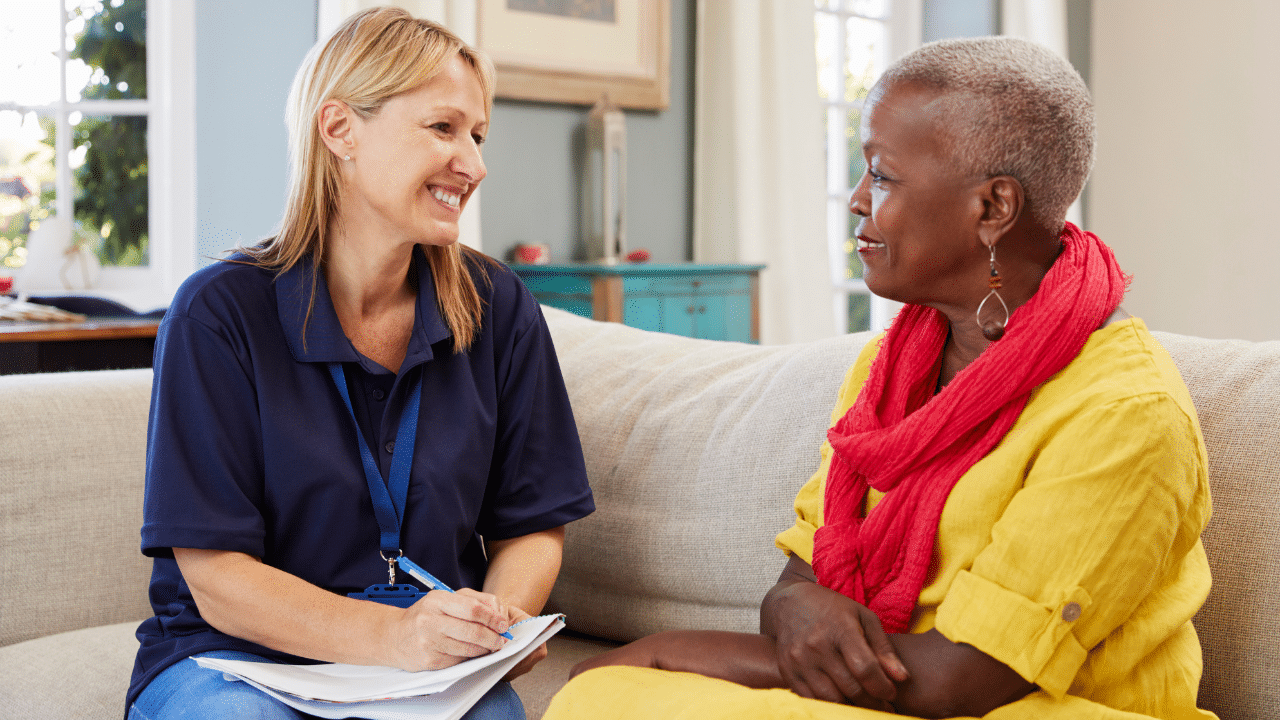
As professionals working with older adults, particularly those with minoritized identities, it is critical to create an environment that promotes healing, dignity and respect. This can be achieved through combining the practices of trauma-informed care (TIC) and cultural humility (CH).
TIC acknowledges the profound impact of trauma on individuals’ physical, mental and emotional well-being, while CH embraces the diversity of experiences, values and identities that shape each person’s journey. Weaving these principles into practice allows us to provide compassionate care that addresses the unique needs of older adults, honors their lived experiences, and fosters an environment of safety, trust and empowerment.
Older Adults and Trauma
Research indicates that most older adults have experienced traumatic events, which can have lasting effects on their well-being, including PTSD and stress reactions. Estimates of prevalence rates of PTSD in older adults range from 1% to 10%, and PTSD symptoms in older adults may manifest differently than in younger populations.
Stress reactions include heightened anxiety, hypervigilance, intrusive thoughts or emotional distress related to past traumas. Recognizing the unique impact of trauma on minoritized older adults is essential to providing compassionate and culturally responsive care. These folks often face many compounded challenges stemming from systemic oppression, discrimination, and social inequalities. Trauma in the context of their intersecting identities can have a profound and lasting impact on their well-being.
The Role of Resilience in the Lives of Older Adults
Resiliency, or the ability to bounce back, cope, and recover from adversity, including the harmful effects of trauma, in older adults and specifically in minoritized elders, is a remarkable aspect of human strength and adaptability. Research has shown that older adults, despite challenges and traumas, often demonstrate resilience in the face of adversity. Such resilience can be attributed to accumulated life experiences, knowledge, skills and wisdom, which can provide a strong foundation to draw upon, enabling them to navigate difficult circumstances.
Resilience takes on a unique significance in minoritized older adults. The experiences of navigating systemic oppression, discrimination and social inequalities require additional strength and adaptability. Community solidarity, cultural pride and a sense of identity play crucial roles in fostering resilience among such elders. Cultivating a positive cultural identity, engaging in cultural practices, and connecting with one’s community can provide a sense of empowerment and protective factors against the harmful effects of trauma.
Trauma-Informed Care and Cultural Humility
TIC recognizes the widespread impact of trauma and seeks to address it by creating a safe, empowering and healing environment for patients. CH emphasizes the need for healthcare providers to approach patients with an open and respectful attitude, recognizing that each patient’s cultural background and beliefs shape their health and well-being. These frameworks share the common goal of promoting patient-centered care that is sensitive to individual needs and experiences.
Trauma-Informed Care
TIC is based on six core tenets that guide healthcare providers in delivering care that is sensitive to the unique needs and experiences of trauma survivors:
-
- Safety: Patients’ physical safety should be prioritized, but also the environment must feel emotionally safe for patients to share experiences.
- Trustworthiness and Transparency: Healthcare providers should communicate clearly and consistently and avoid making promises they cannot keep.
- Peer Support: Healthcare providers should create opportunities for trauma survivors to connect with others who have had similar experiences and provide opportunities for peer support.
- Collaboration and Mutuality: Healthcare providers should involve patients in decision-making, respect their autonomy, and together develop care plans responsive to patients’ needs.
- Empowerment, Voice and Choice: Healthcare providers should support patients in making informed decisions about their care and encourage them to express their needs and preferences.
- Cultural, Historical and Gender Issues: Healthcare providers should be aware of the cultural and historical context in which the trauma occurred and be sensitive to the ways in which gender and power dynamics may affect the healing process.
Cultural Humility
CH emphasizes self-reflection, openness and a willingness to learn about and work with individuals from diverse cultural backgrounds. It recognizes the importance of recognizing and addressing power imbalances in healthcare settings, and strives to promote equity and inclusivity in care:
-
- Practice lifelong learning and critical self-reflection.
- Recognize and challenge power imbalances, including those related to race, ethnicity, language, gender, sexuality, and socioeconomic status.
- Build and maintain trust.
- Use respectful communication.
- Employ collaborative partnerships.
- Recognize and address bias.
- Be flexible and responsive to the needs and preferences of older adults and families.
- Create cultural safety and an inclusive environment.
Benefits of Trauma-Informed Care and Cultural Humility
By integrating TIC and CH in healthcare systems, we create an environment that promotes healing, empowerment and cultural responsiveness. Some expected benefits:
- Enhanced Client Engagement and Trust: When clients perceive their healthcare providers as sensitive to their cultural needs and traumatic experiences, it leads to increased engagement and trust in the therapeutic process (see also Gopalan et al., 2019).
- Improved Treatment Outcomes: TIC and CH approaches lead to better symptom reduction, improved functioning, and increased client satisfaction.
- Reduced Disparities and Inequities: By recognizing the impact of systemic oppression, discrimination and social determinants of health on clients’ well-being, we can work toward reducing healthcare disparities and inequities and better outcomes.
- Enhanced Cultural Competence: By engaging in CH practices, we can expand our understanding of diverse cultural beliefs, values and practices, leading to improved interactions with clients from different backgrounds.
- Improved Organizational Culture and Well-being: TIC and CH contribute to improved staff satisfaction, reduced burnout, and increased organizational resilience.
TIC and CH: A Case Study
Ms. Thompson is a 75-year-old Black woman seeking therapy to address emotional distress and recurring nightmares related to childhood sexual trauma. She has never received formal treatment for this trauma, carrying the burden silently for decades. A recent move into a new community preceded the onset of symptoms. Ms. Thompson was a middle school educator for 40 years and attended a segregated elementary school. She was actively involved in her local African Methodist Episcopal (AME) Church until she moved and is struggling to find a new church home. What follows is one methodology for addressing her current situation. The following is an example of how Trauma Informed Care (TIC) and cultural humility (CH) principles might be used to provide mental health care to Ms. Thompson.
- Establish Safety & TrustEstablishing safety and trust is paramount when forming a therapeutic connection. As caring professionals, we must acknowledge the intersecting impact of trauma and systemic racism on Ms. Thompson’s life, while validating her struggles in navigating racial and sexual trauma with CH. By prioritizing consent, respecting boundaries, and effectively communicating confidentiality and privacy policies, we can create a secure space where Ms. Thompson feels empowered to share her experiences within TIC. Active listening, empathy, and validation are fundamental in developing a sense of security and honoring the ways in which trauma has been experienced in Ms. Thompson’s life.
- Recognize & Challenge Power ImbalancesAs healthcare providers, we must also recognize and challenge power imbalances in society and healthcare settings, considering race, ethnicity, language, gender, sexuality and socioeconomic status. With CH, we must acknowledge the significance of understanding the cultural, historical and gender contexts that have shaped Ms. Thompson’s traumatic experience.When aware of these dynamics, we can be sensitive to how gender and power dynamics may influence her healing process within TIC. It is essential to openly discuss and validate Ms. Thompson’s experiences of marginalization, oppression, and double jeopardy (compounded challenges and disadvantages experienced by individuals who belong to multiple marginalized groups, especially those who face intersecting forms of oppression, such as racism, sexism, homophobia, transphobia, ableism, etc.), while actively involving her as a partner in decision-making processes. Addressing power dynamics is particularly crucial for non-Black providers and men when considering historical racial and gender disparities. By acknowledging and addressing power imbalances (CH), we can ensure her voice is heard and respected during the therapeutic process.
- CollaborateCollaboration with Ms. Thompson is vital, and it involves active listening, valuing her perspectives, and involving her in goal setting (CH, TIC). Respecting her autonomy and involvement in decision-making is crucial, recognizing that she is the expert on her own experience. By acknowledging and valuing Ms. Thompson’s cultural background and experiences (CH), we can foster a sense of connection and trust in therapy (TIC).
- Adapt Evidence-based Trauma Therapies to Be Culturally RelevantIt is crucial to have a keen understanding of how racism and oppression have affected Ms. Thompson’s life and traumatic experiences (CH, TIC). Our role is to validate her experiences, acknowledging the unique challenges she faces as a Black woman survivor of sexual trauma. This can be accompanied by trauma psychoeducation, normalizing Ms. Thompson’s reactions and explaining the wide-ranging effects of childhood sexual trauma within TIC. Simultaneously, trauma psychoeducation helps Ms. Thompson understand that her reactions are normal and not her fault.Incorporate techniques such as storytelling, cultural rituals, art therapy, or narrative therapy. These adaptations allow Ms. Thompson to express herself and process her trauma in a way that aligns with her cultural identities. Identifying Ms. Thompson’s strengths and resilience factors is also essential, as they contribute to her ability to heal from trauma and include aspects of cultural identity and pride.
- Address Our Biases and AssumptionsBeing mindful of our own biases and assumptions and how they might interfere with or influence care can ensure care that is non-judgmental and equitable. Engaging in self-reflection and working to address biases is crucial to providing culturally humble care.
- Commit to Lifelong LearningOur commitment to lifelong learning and ongoing self-education about cultural considerations is paramount in CH. Staying informed about the experiences of Black individuals, the unique needs of Black women experiencing trauma, and the impact of intersecting identities ensures that therapy remains respectful, inclusive and effective. Adapting the therapeutic approach based on feedback and Ms. Thompson’s evolving needs demonstrates our dedication to her well-being and healing within CH and TIC.
The integration of TIC and CH is invaluable in clinical practice, particularly when working with individuals who have been marginalized and excluded from systems. The shared mission of promoting dignity, worth and a sense of belonging among the older adults we serve highlights the importance of prioritizing these principles.
To put these concepts into action, we must continuously engage in ongoing self-reflection, become aware of our own biases and assumptions (as I did with Mr. Davis), seek cultural education, and actively listen to our clients. By doing so, we can transform the healthcare experience and ensure that all individuals, with their complex trauma histories, and rich cultural backgrounds, receive the compassionate and effective care they deserve.
Please Note: Names and identifying details have been changed to protect patient confidentiality.
This article was originally written by Dr. Regina Koepp for American Society on Aging’s Generations Today July-August 2023 Edition, entitled, Building Trust and Healing After Trauma. ASA holds the copyright for this article.

Dr. Regina Koepp is a board certified clinical psychologist, clinical geropsychologist, and founder and CEO of the Center for Mental Health & Aging: the “go to” place for mental health and aging. Dr. Koepp is a sought after speaker on the topics of mental health and aging, caregiving, ageism, resilience, intimacy in the context of life altering Illness, and dementia and sexual expression. Dr. Koepp is on a mission to ensure mental health and belonging for older adults, because every person at every age is worthy of healing, transformation, and love. Learn more about Dr. Regina Koepp here.
Regina Koepp, PsyD, ABPP








































































Want More? Read Our Most Recent Posts


Older adults deserve high quality mental health care.
Therapists deserve the training to provide that care.
")