
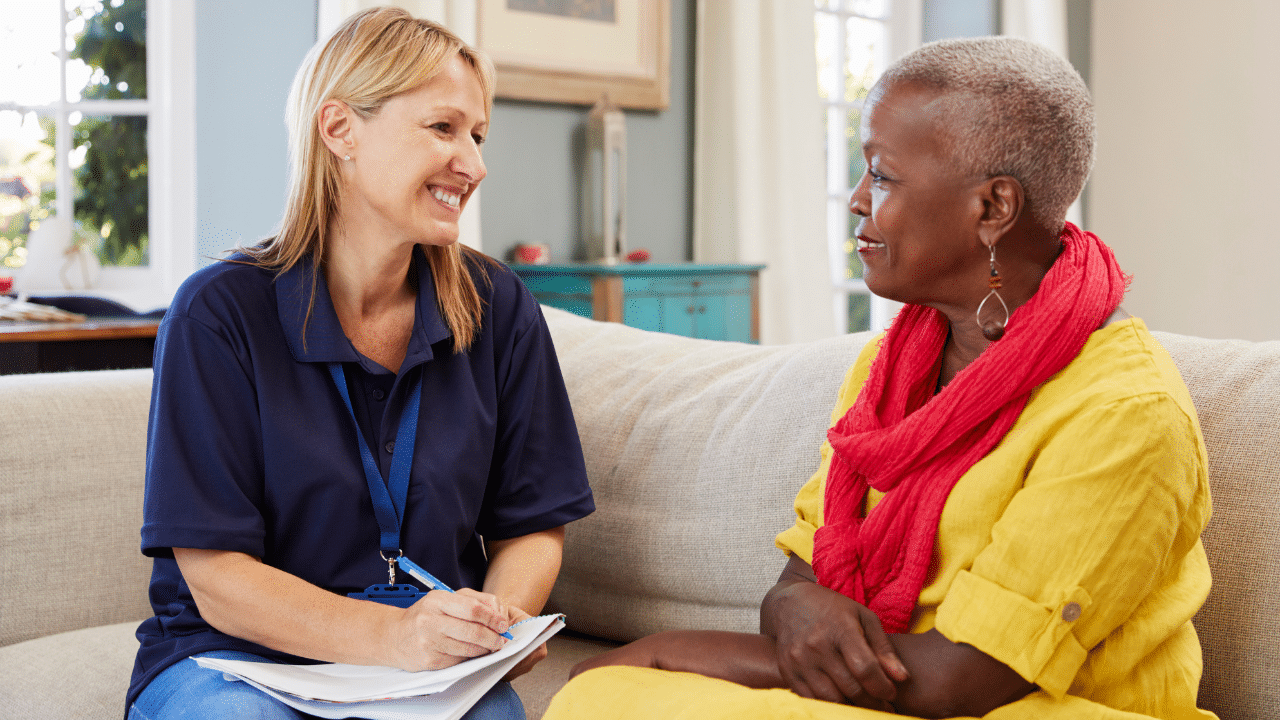
As I write this the wildfires in Los Angeles have displaced more than 100,000 people, and destroyed homes and communities. I’ve heard heartbreaking stories of older adults and people with disabilities unable to leave their homes and evacuate safely. While, at the same time, others have. Imagine you’re working with older survivors of this traumatic event. They’re shaken, struggling to sleep, and can’t seem to stop replaying the event in their mind. You reassure them it’s natural to feel this way after such an ordeal, after all these reactions are a “normal reaction to an abnormal event.”
But what if these feelings don’t fade? What if weeks pass, and their fear starts to take over their daily life?
As mental health professionals, understanding the difference between acute distress that is normal after a trauma versus Acute Stress Disorder (ASD) and a longer-lasting condition like Post-Traumatic Stress Disorder (PTSD) is critical.
This is especially true when working with older adults, who may process trauma differently due to unique life experiences and challenges. Let’s explore what sets these conditions apart and how to support older clients in navigating the aftermath of trauma.
What Are Typical Distress Reactions to Traumatic Events?
Acute distress reactions are the body’s immediate, short-term response to a traumatic event. Think of it as your mind going into overdrive to process what just happened. Symptoms for older adults might include:
Emotional Reactions
- Anxious or fearful
- Overwhelmed by sadness
- Angry
- Guilty, even though he or she had no control over the disaster
- Heroic, able to do anything
- Disconnected, as though he or she doesn’t care about anything or anyone
- Numb, or unable to feel joy or sadness
Physical Reactions
- Having stomachaches or diarrhea
- Having headaches or other physical pain for no clear reason
- Feeling very hungry or not hungry at all
- Sweating or having chills for no physical reason
- Having tremors or muscle twitches
- Feeling jumpy or easily startled
Behavioral Reactions
- Having trouble falling asleep or staying asleep or sleeping too much
- Having increased or decreased energy and activity levels
- Feeling sad or crying a lot
- Using alcohol, tobacco, illegal drugs, or prescription medication in an attempt to reduce distressing feelings or to forget
- Having outbursts of anger
- Having difficulty accepting help or helping others
- Wanting to be alone most of the time and isolating him- or herself
Cognitive Reactions
- Having trouble remembering things
- Having trouble thinking clearly and concentrating
- Worrying a lot
- Having trouble making decisions
- Having trouble talking about what happened or listening to others talk about it
The Key Details of Distress We Expect to See After a Traumatic Event.
- Timing: ASR happens quickly—often within minutes or hours of the event—and typically resolves within a few days to a month.
- Purpose: It’s the body’s way of trying to cope with something unexpected and overwhelming. These are “normal responses to an abnormal event” and often do not require mental health intervention.
Acute Stress Disorder
Acute Stress Disorder is a mental health condition that can occur within the first month following exposure to a traumatic event. It is characterized by a range of symptoms that develop immediately after the trauma and last between 3 days and 4 weeks.
The diagnostic criteria for Acute Stress Disorder (ASD) according to the DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, 5th edition, Text Revision) are as follows:
- Exposure to a traumatic event (directly or indirectly)
- The symptoms cause significant distress or impairment in social, occupational, or other important areas of functioning.
- The symptoms are not attributable to the physiological effects of a substance or another medical condition.
- Presence of 9 or more symptoms from the following 5 categories, lasting for 3 days to 1 month after the traumatic event:
Intrusion Symptoms
- Recurrent, involuntary, and intrusive distressing memories of the event
- Recurrent distressing dreams related to the event
- Dissociative reactions (e.g., flashbacks)
- Intense psychological or physiological distress when reminded of the event
Negative Mood
- Persistent inability to experience positive emotions
Dissociative Symptoms
- Altered sense of reality
- Inability to remember important aspects of the traumatic event
Avoidance Symptoms
- Efforts to avoid distressing memories, thoughts, or feelings associated with the event
- Efforts to avoid external reminders of the event
Arousal Symptoms
- Sleep disturbance
- Irritability or angry outbursts
- Hypervigilance
- Difficulty concentrating
- Exaggerated startle response
It’s important to note that ASD is diagnosed when symptoms last between 3 days and 1 month after the traumatic event. If symptoms persist beyond one month, a diagnosis of Post-Traumatic Stress Disorder (PTSD) should be considered instead
Post-Traumatic Stress Disorder
Post-Traumatic Stress Disorder, on the other hand, is a longer-term condition that can develop after experiencing or witnessing a traumatic event. PTSD is diagnosed when symptoms persist for more than one month and can sometimes emerge months or even years after the initial trauma.
According to the DSM-5-TR, the diagnostic criteria for Post-Traumatic Stress Disorder (PTSD) are as follows:
Criterion A: Stressor
Exposure to actual or threatened death, serious injury, or sexual violence in one or more of the following ways:
- Direct exposure to the traumatic event
- Witnessing the trauma as it occurred to someone else
- Learning about a close family member or friend being exposed to trauma
- Indirect exposure to aversive details of the trauma (e.g., first responders)
Criterion B: Intrusion Symptoms
Presence of one or more of the following intrusion symptoms associated with the traumatic event:
- Recurrent, involuntary, and intrusive distressing memories
- Recurrent distressing dreams related to the event
- Dissociative reactions (e.g., flashbacks)
- Intense or prolonged psychological distress at exposure to cues
- Marked physiological reactions to reminders of the event
Criterion C: Avoidance
Persistent avoidance of stimuli associated with the traumatic event, evidenced by one or both of:
- Avoidance of distressing memories, thoughts, or feelings about the trauma
- Avoidance of external reminders that arouse distressing memories, thoughts, or feelings
Criterion D: Negative Alterations in Cognitions and Mood
Negative alterations in cognitions and mood associated with the traumatic event, evidenced by two or more of:
- Inability to remember important aspects of the trauma
- Persistent and exaggerated negative beliefs about oneself, others, or the world
- Persistent, distorted cognitions about the cause or consequences of the trauma
- Persistent negative emotional state
- Markedly diminished interest in significant activities
- Feelings of detachment or estrangement from others
- Persistent inability to experience positive emotions
Criterion E: Alterations in Arousal and Reactivity
Marked alterations in arousal and reactivity associated with the traumatic event, evidenced by two or more of:
- Irritable behavior and angry outbursts
- Reckless or self-destructive behavior
- Hypervigilance
- Exaggerated startle response
- Problems with concentration
- Sleep disturbance
Criterion F: Duration
Persistence of symptoms in Criteria B, C, D, and E for more than one month
Criterion G: Functional Significance
The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning
Criterion H: Exclusion
The disturbance is not attributable to the physiological effects of a substance or another medical conditionAdditionally, the DSM-5-TR includes two specifiers for PTSD:
- With dissociative symptoms (depersonalization or derealization)
- With delayed expression (full diagnostic criteria are not met until at least 6 months after the trauma)
Here’s a table differentiating Acute Stress Disorder (ASD) from Post-Traumatic Stress Disorder (PTSD):
| Feature | Acute Stress Disorder (ASD) | Post-Traumatic Stress Disorder (PTSD) |
| Onset | Within 3 days to 1 month after trauma | At least 1 month after trauma; can develop months or years later |
| Duration | 3 days to 1 month | More than 1 month; can persist for months or years |
| Key Symptoms | Dissociative symptoms, anxiety, emotional numbing, flashbacks | Re-experiencing trauma, avoidance, negative mood/cognition changes, hyperarousal |
| Diagnostic Criteria | Based on total number of symptoms present | Requires meeting specific symptom criteria within established clusters |
| Treatment Duration | Short-term interventions | Long-term therapy often required |
| Typical Treatments | Brief cognitive-behavioral therapy, crisis management; Psychological First Aid | Prolonged exposure therapy, cognitive processing therapy, medication management, EMDR, Somatic therapies |
| Evolution | Can potentially lead to PTSD | Does not lead to ASD |
| Dissociative Symptoms | More prominent | Less prominent; included as a subtype |
| Negative Mood Symptoms | Less prominent | More prominent and varied |
| Risk of Chronic Issues | Lower | Higher |
This table highlights the main differences between ASD and PTSD in terms of onset, duration, symptoms, diagnosis, treatment, and other key features
Treatment Approaches
While there is some overlap in treatment strategies, the approaches for ASD and PTSD can differ:
- ASD: Treatment typically involves short-term interventions, such as Psychological First Aid, brief cognitive-behavioral therapy (CBT), and crisis management.
- PTSD: Treatment often requires longer-term psychotherapy, such as prolonged exposure therapy, cognitive processing therapy, EMDR, somatic therapies, and may include medication management
Special Considerations for Older Adults
According to the National Center for PTSD, up to 90% of adults aged 65 and up have been exposed to at least one potentially traumatic event during their lifetime.
The prevalence of current Post Traumatic Stress Disorder (PTSD) in adults over 60 ranges from 1.5% to 4%. Although many older adults do not meet full criteria for a PTSD diagnosis, about 7%-15% of older adults exhibit sub-clinical levels of PTSD symptoms.
While PTSD is a mental health condition immediately attributed to exposure to trauma, other mental health conditions can also be associated with exposure to trauma, including:
- Anxiety disorders
- Depressive disorders
- Substance use disorders
- Psychosis
- Suicidality
- Borderline personality disorder
1. PTSD can increase with age.
- Role changes and loss of independence may make coping with memories of earlier trauma more challenging.
- Increase in stressors like retirement, health problems, decreased sensory abilities, reduced income, loss of loved ones, decreased social support, cognitive impairment, etc
- Coping strategies used to manage post-traumatic stress symptoms in early and mid-life (e.g., over working or substance use), may be less effective or available in older adulthood.
- PTSD symptoms may be more severe in people with cognitive impairment and dementia disorders, which disproportionately impacts older adults.
2. Lifetime Exposure to Trauma
Older adults have a higher likelihood of experiencing multiple traumatic events throughout their lives. Studies show that up to 90% of older adults have been exposed to at least one traumatic event in their lifetime. This cumulative trauma exposure can complicate the presentation and treatment of ASD and PTSD among older adults.
3. Delayed Onset or Resurgence of Symptoms
For some older adults, PTSD symptoms may emerge or resurface later in life, even if they have not previously shown signs of the disorder. Life changes associated with aging, such as retirement or health issues, can trigger or exacerbate symptoms of past trauma.
4. Unique Symptom Presentation
Older adults may express trauma-related symptoms differently compared to younger individuals:
- Physical complaints: Older adults may be more likely to report physical symptoms such as pain, sleep disturbances, or gastrointestinal issues rather than emotional distress
- Cognitive concerns: Older adults might focus on cognitive difficulties or memory problems, which can sometimes be mistaken for signs of dementia
5. Comorbid Health Conditions
Older adults with ASD or PTSD often have co-occurring physical health conditions. Research has shown that PTSD is associated with an increased risk of chronic health problems, including hypertension, cardiovascular issues, and arthritis. These comorbidities can complicate both assessment and treatment.
6. Cognitive Impairment and Dementia
Studies suggest that severe and prolonged trauma or a history of PTSD may increase the risk of cognitive decline and dementia in older adults. This relationship highlights the importance of early intervention and comprehensive care for trauma-related disorders among older adults.
7. Treatment Considerations
When treating older adults with ASD or PTSD, several factors should be taken into account:
- Holistic approach: Treatment should address not only the trauma-related symptoms but also consider the overall physical and mental health of the individual.
- Medication sensitivity: Older adults may be more sensitive to medication side effects and are often managing multiple medications for various health conditions
- Adaptations to psychotherapy: While evidence-based treatments like Cognitive Processing Therapy (CPT) and Prolonged Exposure (PE) can be effective for older adults, some modifications may be necessary to accommodate age-related factors
Assessment and Screening for PTSD in Older Adults
Proper assessment and screening for ASD and PTSD in older adults are crucial for effective treatment. Here are some key points to consider:
- Routine screening: Assessment of trauma and related symptoms should be a routine part of healthcare for older adults. And, can easily be included in primary care visits. Here is a Primary Care PTSD Screen for PTSD (5-questions).
- Comprehensive psychological evaluation: When indicated, mental health providers should conduct a thorough evaluation that includes both physical and mental health assessments, given the complex interplay between trauma, aging, and overall health.
- Trauma Assessment Tools Normed with Older Adults: Many trauma and PTSD assessment measures have been validated for use with older adults. However, clinicians should be aware of potential age-related factors that may influence test results.
- This includes the Clinician-Administered PTSD Scale (CAPS)
- The gold standard in structured diagnostic interviews, and the self-report PTSD Checklist.
- Suicide risk assessment: Older adults, particularly older men, are at increased risk for suicide, making thorough suicide risk assessment crucial.
Prevention and Intervention Strategies
When it comes to preventing and addressing trauma-related challenges in older adults, a well-rounded, compassionate approach is key. Here’s how you can make a difference:
- Start Early: The sooner we recognize and address signs of Acute Stress Disorder (ASD), the better the chances of preventing it from turning into PTSD. Sometimes, a little early support can go a long way.
- Share Knowledge: Educating older adults—and their caregivers—about how trauma can affect them and offering simple coping strategies can be empowering. Plus, when people understand what’s happening, they feel less alone, and the symptoms can feel less overwhelming.
- Build Connections: Strengthening social support is a game-changer. Whether it’s reconnecting with friends, joining a group, or leaning on family, having a strong network makes recovery so much easier.
- Personalize Care: Older adults have unique stories, physical needs, and cognitive abilities that shape how they experience and heal from trauma. Tailoring treatments to their individual circumstances ensures they get the care and attention they truly need.
By combining these strategies, we can help older adults not just recover but thrive, even in the face of trauma.
Wrapping It All Up
Trauma can impact anyone, but for older adults, the journey through recovery is shaped by a lifetime of experiences, unique challenges, and incredible resilience. Whether it’s understanding the difference between Acute Stress Reaction (ASD)and PTSD or finding the best ways to offer support, what we do as professionals matters deeply.
Every conversation you have, every resource you share, and every bit of care you provide has the potential to change a life. By staying informed and compassionate, you’re not just helping someone heal—you’re helping them rediscover their strength and joy.
As we wrap up, I invite you to keep the momentum going. Download our Trauma-Informed Care Guide today and take one more step toward becoming an even stronger advocate for older adults. And don’t forget to share this with a colleague—it’s only together that we can truly meet the mental health needs of older adults.
Helpful Resources
- Helping Older Adults After Disasters: A Guide by SAMHSA
- Helping Older Adults Prepare for Disasters: Essential Resources & Tips
- Trauma-Informed Care Guide for Older Adults: Download here
- SAMHSA Disaster Distress Helpline: 1-800-985-5990
- National Crisis Hotline for Mental Health: Call 988 (Like 9-1-1 but for mental health emergencies)

Dr. Regina Koepp is a board certified clinical psychologist, clinical geropsychologist, and founder and CEO of the Center for Mental Health & Aging: the “go to” place for mental health and aging. Dr. Koepp is a sought after speaker on the topics of mental health and aging, caregiving, ageism, resilience, intimacy in the context of life altering Illness, and dementia and sexual expression. Dr. Koepp is on a mission to ensure mental health and belonging for older adults, because every person at every age is worthy of healing, transformation, and love. Learn more about Dr. Regina Koepp here.
Regina Koepp, PsyD, ABPP







































































Want More? Read Our Most Recent Posts


Older adults deserve high quality mental health care.
Therapists deserve the training to provide that care.
")