
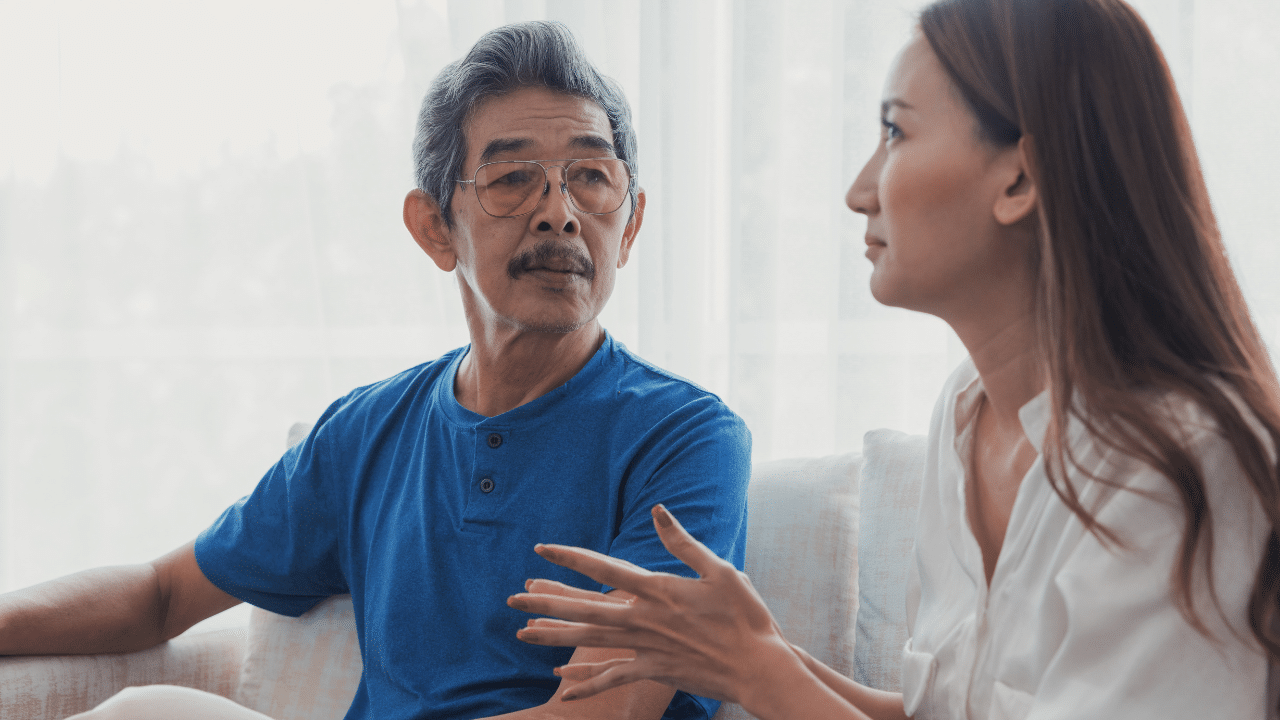
The plan was already made. The family had toured the memory care facility twice, signed the paperwork, and arranged for movers to collect her things the following week. But when they pulled into the parking lot, her daughter told her she would just be staying for a few days while her back healed up.
She brought one small bag.
That was eight months ago. Her daughter still can’t get through a session without circling back to that parking lot. Not because the move was wrong — her mother needed that level of care, and everyone involved knew it. But because of the words just a few days. Because her mother had looked at her and said, “Okay” and trusted her completely.
That kind of guilt doesn’t dissolve when the dust settles. It compounds.
This scenario is more common than most people realize, and the question it raises — Was lying the right thing to do? — doesn’t have a clear answer. But the evidence does give us important guardrails.
In this article, I’ll share some research on what we know about deception, relocation, and dementia care — including when limited deception might reduce harm, and when it almost certainly makes things worse.
What Is “Therapeutic Lying” in Dementia Care?
In dementia care, “therapeutic lying” — sometimes called therapeutic fibbing or creative communication — refers to using gentle untruths to reduce distress when correcting someone’s reality causes more harm than good (Day et al., 2011). Think of telling someone that her husband is “at work” rather than explaining, again, that he died fifteen years ago, only to have them experience the raw, fresh grief as a daily experience.
Most ethicists who engage with this practice DO NOT favor deception, at the same time, they recognize that in moderate-to-severe dementia, it may sometimes be the least harmful option when safety and recurrent distress are at stake (Day et al., 2011).
When it comes to using deception to move, the focus should be in what causes the least harm.
The bulk of the literature on therapeutic lying focuses on small, day-to-day interactions — not major life events like a permanent relocation. When the deception involves something as significant as leaving home forever, the stakes are considerably higher.
“Therapeutic fibbing” was never designed as a relocation strategy. The evidence base for it is narrow, and the risks of applying it to a forced move are substantial.
Transfer Trauma: What Happens When a Move Goes Wrong
Before we can talk about deception, we have to talk about how relocation itself can impact older adults.
Transfer trauma (also called relocation stress syndrome) is a well-documented phenomenon in geriatric care. Moving from one’s home to a long-term care or memory care setting is one of the most disorienting experiences a person can go through — and the research reflects that (Bekhet et al., 2009).
Common reactions include:
- Anxiety, confusion, and depression
- Sleep disturbance and withdrawal
- Increased agitation and behavioral changes
- Refusal of care
- Decline in physical and cognitive functioning
These outcomes are significantly worse in involuntary moves, moves with little preparation, and moves where the person feels excluded from the decision (Bekhet et al., 2009). Deception, by definition, removes the opportunity for the older person to be a part of the decision- called shared decision-making- and denies them the opportunity to prepare emotionally for this significant transition.
When deceit is layered on top of an already-difficult relocation, the psychological impact doesn’t just stay the same — it compounds. A person who might have eventually adjusted to a new setting now has an additional wound to contend with: the betrayal of being lied to and the complex bind of being a position in which they rely on that person for assistance and guidance with ruptured trust.
The Pros and Cons of Lying About A Move to Memory Care
I’m not going to tell you that deception around a move is always wrong and never discuss it further. That would be dishonest, and it wouldn’t serve the families and clinicians who face these decisions in real time. So let’s explore both sides: the pros and cons of lying about a move to memory care.
When limited deception might reduce harm
There are narrow circumstances where ethical analysts have recognized that some deception may be defensible:
-
Moderate-to-severe dementia with minimal capacity for consent:
- When someone cannot process complex information even after repeated, gentle explanations, and is at imminent risk (frequent falls, wandering, agitation), a simple, non-frightening framing may reduce immediate distress more than a detailed reality check would.
-
Time-limited framing that is partly true:
- Presenting a move as a “trial stay” or “short-term rehab” might be ethically acceptable if there is a genuine intention to reassess — and if the framing isn’t an elaborate fiction but a simplified version of a real possibility (Kadish, 2007).
-
When honest communication predictably causes unrelievable harm:
- If repeated truthful explanations consistently produce intense agitation, self-harm threats, or severe behavioral disturbance that can’t be safely managed, limited therapeutic fibbing may serve as a harm-reduction measure.
Even in these circumstances, the literature emphasizes proportionality and last resort — after truthful, simplified, empathic communication and environmental supports have been tried and failed (Day et al., 2011).
When deception almost certainly causes harm
Far more commonly, deception around a move does real damage:
-
When cognition is relatively intact:
- For older adults with mild cognitive impairment or no significant impairment, discovering they were deceived about leaving home can produce lasting anger, resentment, and broken trust in family and professionals. Research on relocation consistently shows that feeling excluded from decisions worsens distress and adjustment (Deber et al., 2007).
-
When motivated by convenience:
- Using deception primarily to avoid a hard conversation or speed up a discharge — rather than to genuinely relieve the older person’s suffering — is not supported by any ethical analysis of dementia care.
-
When less-restrictive options haven’t been tried:
- Evidence-based practice for dementia transitions emphasizes early education, incremental involvement, and honest communication before any move is made (Alzheimer’s Association, 2018). Skipping those steps and going straight to deception undermines person-centered care.
-
When there is a history of trauma or institutional mistrust:
- People with prior trauma or deep distrust of systems are especially vulnerable to discovering they’ve been misled. Resulting in escalated distress, behavioral symptoms, refusal of care, and physical and cognitive decline.
The Psychological Impact — on Everyone
On the older adult
Beyond the standard transfer trauma reactions, deceit adds:
- Betrayal and humiliation when they later understand they were misled — which can manifest as anger, suspiciousness, depression and withdrawal, or refusal to engage with family or staff
- Heightened “who can I trust?” anxiety, which is particularly destabilizing in dementia, where the internal world already feels uncertain
- Worsened behavioral symptoms — mistrust can translate into resistance to care, accusations, or paranoid ideation
- Ambiguity and difficulty adjusting due to lack of clarity: “you told me I would only be here for a few days, it’s been 8 months, when am I going home?”
These presentations are sometimes addressed symptomatically — with medication or behavioral interventions — without ever identifying deception-related betrayal as the underlying cause.
On the family caregivers
Family caregivers who have used deception around a move consistently describe:
- Intense guilt and sadness, even when they believe they had no other option
- Cognitive dissonance and moral distress between lifelong values about honesty and what they actually did
- Fear of judgment from siblings, professionals, or their broader community
- Relief that their loved one is safe, mixed with grief at the loss of the former relationship
Moral distress is the painful psychological tension that arises when you know what feels right — but find yourself unable to act on it, or worse, find yourself doing something that conflicts with your deepest values, and feel out of alignment with your moral integrity.
Moral distress is highest when people feel forced by system constraints — unsafe discharge pressures, lack of community resources — and when family members are not aligned with each other about the approach (Teno et al., 2011).
The caregiver’s guilt doesn’t go away just because the move was necessary. Moral distress needs to be processed — not just explained away.
Evidence-Based Alternatives to Deception
The research on dementia care transitions is fairly consistent: honest, person-centered, well-planned transitions produce better outcomes than those built on deception — for the older adult and for the family. Here’s what that actually looks like.
1. Honest (but gentle) communication
- Use simple, repeated explanations focused on needs and benefits rather than deficits: “This place has people who can help with your walking and medicines so you stay safer.”
- Validate emotions first — “I know you love your home, and this is really hard” — before providing information
- Offer choices where possible: timing of the move, which possessions to bring, how the room is arranged. Even these types of choices support autonomy.
2. Involve medical providers
Having a trusted clinician — primary care, neurologist, geriatrician — discuss safety and care needs directly often lends credibility and reduces the sense that “my children just want to get rid of me.” Evidence-based transitional care models stress coordinated communication among the individual, the caregiver, and the clinical team about upcoming transitions and their rationale. Family members can attend visits (with consent) to share observations about falls, confusion, or caregiver strain, allowing the clinician to make strong, specific recommendations.
3. Early and gradual planning
Successful dementia transition programs educate individuals and caregivers early about likely future transitions and how to delay or avoid them — and they involve both parties in planning (Alzheimer’s Association, 2018). Introducing the idea of extra help, adult day programs, respite stays, and trial stays can normalize the full spectrum of supports and reduce the shock of a sudden, permanent move.
4. Explore less-restrictive options first
Before any move, evidence-based practice calls for exploring home modifications, in-home care, adult day programs, medication management supports, and technology to reduce risk (Alzheimer’s Association, 2018). When these supports are tried first — and when they eventually prove insufficient — both families and older adults often have an easier time accepting that “we really did try everything we reasonably could.”
5. Use structured transition programs
Models like adaptations of the Transitional Care Model and dementia caregiver training programs bring together the most effective elements: education about transitions, timely communication, involvement of the person with dementia in planning, and emotional support for caregivers before and after the move (Naylor et al., 2011).
Aging Life Care Professionals (formerly known as Geriatric Care Managers), dementia-capable social workers, and interdisciplinary teams can help implement or approximate these approaches in community settings.
Putting It Together: A Practical Framework
For a specific family navigating this decision, here’s the sequence the evidence supports:
- Assess capacity and insight carefully, often with neuropsychological and medical provider input.
- Try repeated, honestly framed, gently delivered conversations that validate feelings and offer concrete reasons and benefits.
- Involve trusted clinicians to explain risks and recommendations; consider joint visits.
- Explore and trial less-restrictive supports first (if appropriate and safe).
- If — after all of these steps — the person still cannot understand or accept the move and is at significant risk due to dementia and lack of insight, consider narrow, proportionate therapeutic fibbing aimed at minimizing distress during the transition. Maintain as much honesty and person-centeredness as possible, and attend to your own emotional needs throughout.
Across all the literature, the through-line is this: respect for autonomy, preparation, honest communication, and caregiver support are the core of ethical transitions. Deception, if used at all, should be considered a last-resort measure — not a default strategy and not a shortcut (Alzheimer’s Association, 2018).
Deception might sometimes be the least-bad option. It is never the best option.
A Note for Clinicians + Therapists
The families I work with who have used deception to move a loved one are not bad people making careless choices. They are exhausted, frightened people who often felt they had no other option — sometimes because the system gave them no real alternatives, and sometimes because no one had helped them think through what other options existed.
Our job, as clinicians, is to get in earlier. To help families have these conversations before the crisis forces their hand. To offer the psychoeducation, the communication strategies, and the emotional support that makes a more honest path possible. And when families come to us afterward, carrying guilt that doesn’t lift — our job is to sit with that, to help them understand the ethics they were navigating, and to support the healing that still needs to happen.
This is hard work. It’s also some of the most important work we do. So, thank you for doing it.
Related Courses & Continuing Education
If this article resonated with you, join me for my upcoming course on Therapy Across the Stages of Dementia from Individual to Caregiver Family Therapy (6 CE Credits)

Related Articles
- Therapy for Families and Individuals Following a Difficult Move to Memory Care
- Transfer Trauma in Older Adults: Relocation Stress, Identity Loss, and How Therapy Can Help
- Separation Anxiety in Older Adults: What Every Clinician Needs to Know
- Aging Parent Calling Too Many Times a Day? 5 Next Steps
- Do Caregivers Really Die Before Their Loved Ones? What The Science Actually Says
- Grieving Someone Who’s Still Alive: Understanding Ambiguous Loss

Dr. Regina Koepp is a board certified clinical psychologist, clinical geropsychologist, and founder and CEO of the Center for Mental Health & Aging: the “go to” place for mental health and aging. Dr. Koepp is a sought after speaker on the topics of mental health and aging, caregiving, ageism, resilience, intimacy in the context of life altering Illness, and dementia and sexual expression. Dr. Koepp is on a mission to ensure mental health and belonging for older adults, because every person at every age is worthy of healing, transformation, and love. Learn more about Dr. Regina Koepp here.
Regina Koepp, PsyD, ABPP







































































Want More? Read Our Most Recent Posts


Older adults deserve high quality mental health care.
Therapists deserve the training to provide that care.
")