
Living alone is a choice many of us treasure—the independence, the comfort of familiar surroundings, the dignity of managing our own daily rhythms. But what happens when dementia enters this picture?
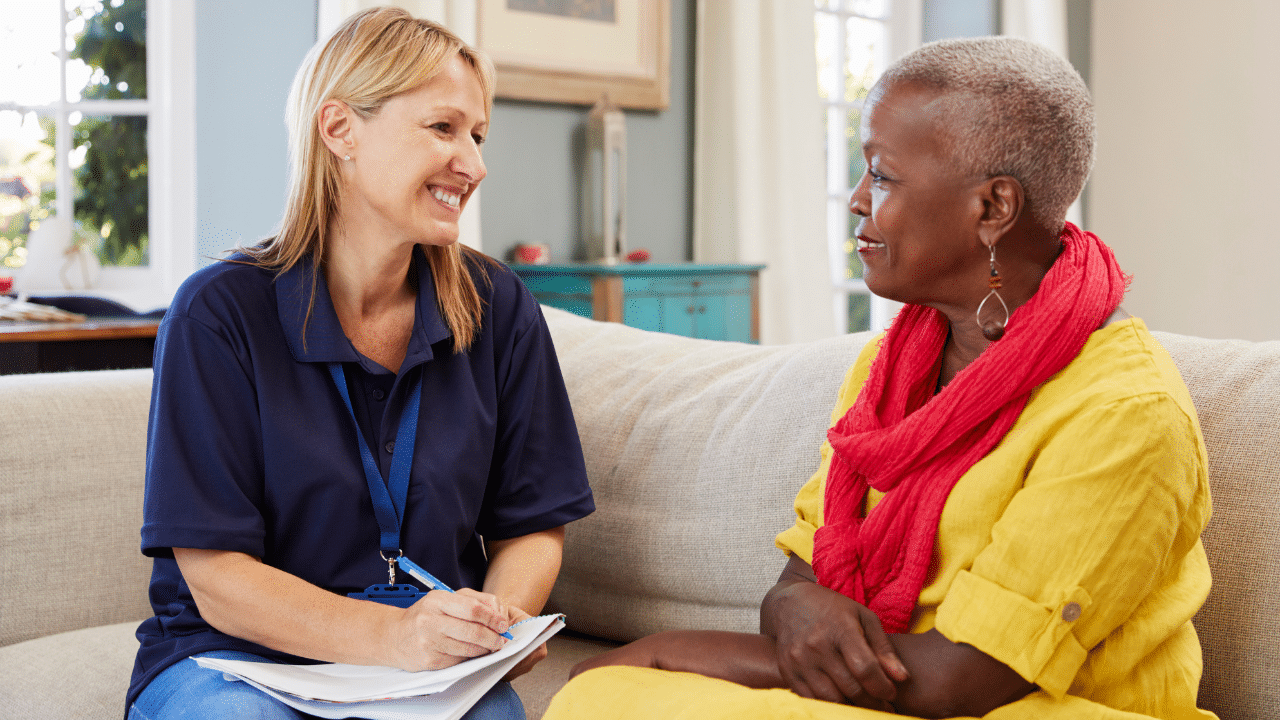
As a geropsychologist who has worked with thousands of older adults navigating cognitive changes, I’ve witnessed both the profound challenges and the remarkable resilience of people with dementia who live alone without a readily available support network.
Today, I want to share insights from a comprehensive handbook developed by RTI International for the Administration for Community Living that addresses this often-overlooked population.
Whether you’re a healthcare professional, social worker, neighbor, or concerned community member, understanding how to recognize and respond to the needs of people living alone with dementia can make a life-changing difference.
The Reality of Living Alone with Dementia
The numbers tell an important story: research indicates that approximately 36.0% of U.S. adults 65+ with probable dementia were living alone (Singer, Nelson, & Menne, 2025), and is expected to increase in the coming years.
While many have caregivers nearby, some truly do not—and these individuals face heightened risks for self-neglect, malnutrition, medication errors, financial exploitation, and social isolation.
What makes this particularly concerning is that people with dementia who live alone are much less likely to have been diagnosed with the condition and are less likely to recognize their own limitations or seek help (Lehmann et al., 2010). It’s a crisis hiding in plain sight within our communities.
Why Someone Might Be Alone
Before we jump to assumptions, it’s important to understand that people with dementia live alone for various reasons:
- Personal choice: Some individuals have always valued independence and prefer living alone
- Life circumstances: Outliving family and friends is an unfortunate reality for many older adults
- Temporary situations: A caregiver may be hospitalized or dealing with their own health crisis
- Unexpected loss: The sudden death or nursing home placement of a spouse or primary caregiver
- Family dynamics: Sometimes family members have chosen to discontinue contact, or they may be unable to provide meaningful support due to their own challenges
Understanding the “why” helps us approach each situation with empathy rather than judgment.
The Delicate Balance: Safety and Autonomy
Here’s the ethical dilemma that keeps professionals like me and you awake at night: How do we balance respecting an individual’s right to live independently with ensuring their safety?
The truth is, there’s no perfect environment for someone with dementia living alone. A certain amount of risk is inevitable.
Our role isn’t to eliminate all risk—that’s impossible and would require removing someone’s fundamental autonomy—but rather to thoughtfully assess risks and creatively explore interventions that are the least restrictive possible.
This means we need to ask ourselves:
- Can we add safeguards without removing independence?
- Can we provide support that honors dignity while addressing genuine safety concerns?
Assessing Risk: What to Look For
When I evaluate someone with dementia who’s living alone, I consider several key factors using a framework I call “SHARP”:
- Safety: What safety issues are affected by the person’s condition?
- Hazards / Risks: What specific risks does this individual face?
- Abilities/Capacity: What can (and cannot) the person do for themselves?
- Resources/ Aids: What supports, technology, or modifications could mitigate these risks?
- People/Programs/Services: What individuals, programs, and services can we mobilize?
Critical Safety Considerations
Wandering and Getting Lost:
When I work with families, I often say, “people with dementia don’t wander, until they do, it’s important to have a plan in place.”
While it’s hard to say for sure, the Alzheimer’s Association states that “six in 10 people living with dementia will wander at least once”. And a federal brief (2015) on dementia-related wandering and exit‑seeking notes that “more than half of people with dementia will wander at some point during the course of their disease.”
Unlike someone with a caregiver at home, a person living alone who wanders may not be reported missing for hours or even days. GPS tracking systems, identification bracelets like Medic-Alert + Safe Return, and participation in dementia-friendly community initiatives can help.
Falls and Home Accidents:
Falls are the leading source of in-home injury for people with dementia. Without someone present, a fall can be catastrophic. Fall detectors that automatically call for help, removal of trip hazards, and regular home safety assessments are essential preventive measures.
Nutrition and Hydration:
Research shows that people living alone with dementia are at greater risk for malnutrition than those living with others (Nourhashemi et al., 2005). Home-delivered meal programs like Meals on Wheels can provide not just nutrition but also regular wellness checks.
Financial Exploitation:
This is one of the most common forms of elder abuse affecting people with dementia living alone. The isolation combined with cognitive impairment creates a perfect storm for scammers and even opportunistic family members or “helpers.”
* See resources section below
Finding the Hidden Support System
One of the most important—and often successful—steps we can take is conducting a thorough search for people who care about the individual. You’d be surprised how often a “friendless” person actually has someone willing to help if only they could be located.
Practical Search Strategies
- Review cell phone contacts and recent calls
- Look through address books, holiday cards, and photographs at the person’s home
- Check answering machine or voicemail messages
- Contact past employers (who may have records of emergency contacts)
- Speak with neighbors, faith community members, mail carriers, local shopkeepers.
- Review old legal documents (lawyers can often reach out to contacts without breaching confidentiality)
- Connect with the person’s healthcare providers
- Check with their landlord or building management
Sometimes the person who emerges isn’t a family member at all—it might be a longtime neighbor, a former colleague, or a friend from decades past who would be honored to help.
Decision-Making Capacity: A Nuanced Assessment
Here’s something crucial that many people don’t understand: A diagnosis of dementia does not automatically end a person’s legal capacity to make decisions.
Capacity is both task-specific and time-specific. Someone might be able to express preferences about their daily routine but not have the capacity to execute a complex power of attorney. They might be more lucid in the morning than the evening.
According to established criteria, decision-making capacity requires four abilities:
- Understanding information relevant to the decision
- Appreciating the significance of that information for one’s own situation
- Reasoning with relevant information to weigh options
- Expressing a choice
If there’s any question about capacity, it’s essential to consult with professionals trained in capacity assessment—physicians, neuropsychologists, geropsychologists, or geriatric psychiatrists.
Supported Decision-Making: A Person-Centered Approach
Supported decision-making (SDM) is based on a simple but profound premise: all people, as long as they can make and communicate a choice, have a fundamental right to do so.
In SDM, the person with dementia selects supporters, advisors, and agents who help them:
- Understand questions, issues, and options
- Offer advice
- Express their preferences and choices
It’s completely normal for adults to seek advice when making decisions. SDM simply formalizes this process and provides the legal authority needed for supporters to carry out the person’s choices.
Practical SDM Strategies
Break down support needs into specific areas:
- Home maintenance
- Financial management
- Grocery shopping and meal preparation
- Transportation
- Medication management
- Healthcare decisions
Then identify potential helpers for each area: neighbors, volunteers, social service providers, professional services. An Aging Life Care Professional or care coordinator might be able to help assemble and maintain this support team.
Important note:
Before reaching out to estranged family members, try to understand why relationships are disconnected. We never want to reintroduce someone who brought harm or exploitation into the person’s life and vice versa. If the relationship is estranged because of harm the person living with dementia caused, we must respect the estranged family member’s boundaries.
When Technology Can Help
We’re living in an era where assistive technology can genuinely enhance safety without being intrusive:
- Smart home devices: Gas detectors, water level monitors, temperature alerts
- Medication dispensers: Automated reminders and dispensing systems
- One-touch phones: Simplified calling for emergencies
- Fall detection: Wearable devices that automatically call for help
- Smart locks: Bluetooth or remote access so the person doesn’t get locked out
- GPS trackers: For those at risk of wandering (with the person’s consent)
The key is matching the technology to the individual’s needs and comfort level. What works beautifully for one person might be overwhelming for another.
In dementia care, flexibility is key. It is quite normal to have everything set up and working for a period of time, only for needs and risks to change suddenly.
Financial Protection: A Critical Priority
Financial exploitation is insidious because it often goes undetected until significant damage has been done. Protective strategies include:
- Removing the person from telemarketer lists
- Setting up automatic bill payment
- Designating a trusted third-party contact at banks and utility companies
- Regular credit report checks
- Notifying shopkeepers and bank tellers about the person’s cognitive challenges
- Using professional daily money managers or fiduciaries for complex finances
Here are some helpful resources:
- For Social Security recipients who lack capacity to manage benefits, the Representative Payee program offers oversight without the need for full guardianship.
- For VA Compensation and Pension Benefits– talk with a social worker in your VA primary care clinic about the process for establishing a payee to manage a Veterans finances.
- olderadultnestegg.com – resources for older adults, families, and professionals.
Screening for Abuse and Self-Neglect
This is uncomfortable territory, but we must talk about it. People with dementia living alone are vulnerable to:
- Self-neglect: The most frequently reported concern to Adult Protective Services. Signs include extremely cluttered or dirty living conditions, disconnected utilities, hoarding, not eating, refusing medical care, or dressing inappropriately for weather.
- Financial exploitation: Unusual financial transactions, missing valuables, unpaid bills despite adequate income, sudden changes to wills or powers of attorney.
- Physical or emotional abuse: Unexplained injuries, emotional withdrawal, fear around certain people.
All states have abuse reporting laws. Most licensed professionals are mandated reporters. If you suspect abuse or neglect, you must report it to Adult Protective Services or law enforcement. Getting to know your local APS program can facilitate collaboration and better outcomes.
National Adult Protective Services – APS locator
Guardianship and Conservatorship: The Last Resort
I want to be very clear about this: Guardianship and conservatorship should only be pursued when all reasonable alternatives have been exhausted.
These legal proceedings represent a significant loss of legal rights and personal autonomy. Once these rights are removed, they become incredibly difficult to restore—which is why we must exhaust every other option first.
If you’re working with a family, recommending that they work with an elder care attorney who knows the laws in their specific state is incredibly important. When there is no family, often the state via Adult Protective Services, Public Guardian, or Department of Social Services, or a hospital system may pursue the legal process for Guardianship/Conservatorship.
Understanding the Legal Process
In a guardianship or conservatorship, the court determines whether the person needs protection based on state law standards. Here’s how the process typically unfolds:
- Petition filed: A person or entity (such as a hospital, social worker, or concerned family member) files a petition with the court
- Court investigation: The court conducts an investigation, often including capacity assessments and interviews
- Court determination: If the court determines the individual needs this level of protection, they appoint a guardian or conservator
- Scope defined: The court order specifies exactly what authority the guardian or conservator has
Guardian vs. Conservator: Know Your State’s Terms
Each state has its own legal process, and terminology varies significantly. While most states differentiate between guardian and conservator, others use the terms interchangeably or have entirely different definitions.
General distinctions:
- Guardian = makes personal decisions (healthcare choices, living arrangements, daily care decisions)
- Conservator = manages financial matters (paying bills, managing property, handling assets)
Why this matters: If you’re a professional working in telehealth across state lines, you’ll need to investigate the specific terms and processes for the state where your client resides. What’s called a “guardian” in California might be called a “conservator” in another state, and the legal requirements can differ substantially.
The PRACTICAL Tool: A Framework for Alternatives
Before ever considering guardianship or conservatorship, work through this comprehensive framework developed by the American Bar Association Commission on Law and Aging:
P – Presume guardianship isn’t needed. Start with the assumption that less restrictive alternatives exist. The burden should be on proving guardianship is necessary, not on proving it isn’t.
R – Reason—clearly identify concerns Be specific about what’s actually going wrong.
- Example: Instead of “She can’t manage her life,” identify: “She’s missed three doctor appointments, her utilities were shut off twice, and she’s lost 15 pounds because she’s not eating regularly.”
A – Ask if the condition is temporary or reversible Could this be delirium from a UTI? Medication side effects? Depression following a loss?
- Example: An 80-year-old hospitalized with pneumonia appears confused and can’t make decisions. Rather than immediately pursuing guardianship, treat the infection and reassess—delirium often resolves completely with medical treatment.
C – Community—explore all community-based resources What services exist that haven’t been tried yet?
- Example: Connect with Area Agency on Aging for care management, arrange Meals on Wheels for nutrition, set up automatic bill pay, engage a daily money manager, arrange transportation services, establish regular friendly visitor calls.
T – Team—identify trusted advisors Who in this person’s life could provide support?
- Example: A neighbor who’s willing to check in daily, a former colleague who could help with financial decisions, a niece who lives across the country but could manage things remotely, a church member who could provide transportation.
I – Identify the person’s specific abilities and needs This requires a multidisciplinary assessment. You’ll likely need a team of professionals:
- Occupational/Physical Therapist (functional abilities, safety in home)
- Psychologist or Neuropsychologist (cognitive capacity assessment)
- Social Worker (support systems, community resources)
- Primary Care Provider (medical stability, medication management)
- Geriatric Psychiatrist (if mental health concerns)
Example: Assessment reveals the person CAN make simple daily choices (what to wear, what to eat) and express preferences about relationships, but CANNOT manage complex financial decisions or remember to take medications. This suggests targeted supports (medication management system, financial representative payee) rather than full guardianship.
C – Challenges—address concerns about potential supporters Honestly evaluate whether proposed helpers are appropriate and capable.
- Example concerns: Does the proposed helper have their own substance abuse issues? A history of financial problems? A contentious relationship with the person? Limited availability due to work or distance? If challenges exist, can they be mitigated (co-supporters, oversight mechanisms, bonding) or do we need to find different helpers?
A – Appoint advisors with legal authority Use the least restrictive legal tools available:
- Example: Rather than guardianship, help the person sign a durable power of attorney for finances (with safeguards like required reporting to a third party) and a healthcare power of attorney. Set up a representative payee for Social Security. Establish supported decision-making agreements.
L – Limit any guardianship to only essential issues If guardianship truly becomes necessary, make it as narrow as possible.
- Example: Instead of full guardianship, seek limited guardianship only for financial decisions, preserving the person’s right to make healthcare choices, decide where to live, vote, marry, and make other personal decisions where they retain capacity.
When Guardianship Becomes Necessary
If you’ve worked through the PRACTICAL framework and guardianship or conservatorship is truly the only option, here’s what you should know:
Finding a guardian when no family is available:
Many states offer:
- Public guardian programs: State or local government agencies that serve as guardians
- Volunteer guardian services: Screened and trained community volunteers
- Professional guardians: Private individuals or organizations that serve as guardians for a fee
Keep the scope limited: Even within a guardianship, preserve as many rights as possible. If someone can make healthcare decisions but not financial ones, seek only a conservatorship for finances. If they need help with major medical decisions but can consent to routine care, specify that limitation.
Plan for reassessment: Build in periodic review. Conditions can improve (dementia can be misdiagnosed; treatable conditions can resolve), and guardianships that were once necessary may no longer be needed. Advocate for regular court review of whether the guardianship should continue or be modified.
The goal is always to provide the minimum necessary intervention while maximizing the person’s dignity, autonomy, and self-determination. Guardianship is not a failure—sometimes it’s the most compassionate option—but it should truly be the last resort after every alternative has been thoughtfully explored.
Emergency and Temporary Guardianships: When Crisis Demands Immediate Action
Sometimes situations arise that cannot wait for the standard guardianship process, which can take weeks or months. Two expedited options exist for crisis situations:
Emergency Guardianship/Conservatorship
- When it’s used: When there’s an immediate threat that cannot wait—a person needs emergency surgery but cannot consent, financial exploitation is actively occurring, or severe self-neglect poses an imminent danger.
- Timeframe: Court can grant authority within 24-72 hours, typically lasting only 72 hours to 30 days.
- Important limitation: This addresses only the immediate crisis and does NOT replace the need for a full guardianship hearing if ongoing protection is needed.
- Example: An 82-year-old man with delirium needs emergency hip surgery but has no healthcare power of attorney and cannot understand the consent process. Emergency guardianship allows the surgery to proceed while the court investigates whether permanent guardianship is necessary.
Temporary Guardianship/Conservatorship
- When it’s used: For time-limited situations where someone temporarily cannot manage their affairs—a primary caregiver suddenly dies or is hospitalized, the court needs time to investigate alternatives, or recovery from illness is possible but uncertain.
- Timeframe: Typically lasts 60-180 days and can sometimes be extended.
- Purpose: Serves as a bridge period to stabilize the situation, explore alternatives, and determine if permanent guardianship is truly necessary.
- Example: A woman with moderate dementia has been cared for by her husband, who suffers a sudden heart attack requiring extended hospitalization. Temporary guardianship is appointed for 90 days while the family or entity (e.g., Adult Protective Services, State, or hospital) determines a long-term plan—whether he’ll recover enough to resume caregiving, whether she’ll move near adult children, or whether permanent guardianship is needed.
Critical Safeguards
Because these expedited processes involve reduced due process protections, they must be:
- As narrow in scope as possible (only addressing the specific emergency)
- As brief as necessary (shortest duration that addresses the crisis)
- Never used as a shortcut to bypass full guardianship proceedings when no genuine emergency exists
Use this crisis period wisely: conduct thorough assessments, search for family or supporters, explore less restrictive alternatives, and determine whether permanent guardianship is truly the only option.
If you’re encountering a potential emergency situation, contact Adult Protective Services immediately and seek legal guidance—never attempt to navigate these proceedings alone.
The Power of Community
Ultimately, supporting people with dementia who live alone requires a community response. This includes:
- Dementia-friendly communities that train first responders, business owners, and community members to recognize and assist people with cognitive impairment
- Visiting programs (friendly visitors, home-delivered meals, pet therapy)
- Faith communities and neighborhood networks
- Professional collaboration among healthcare, legal, and social service providers
Practical Resources You Can Access Today
- Dementia Alliance International Created for people with dementia by people with dementia
- Alzheimer’s Association – 24/7 helpline: 1-800-272-3900
- Dementia Friendly America – Building supportive communities
- National Alzheimer’s and Dementia Resource Center
- Aging Life Care Professional – formerly known as Geriatric Care Manager
- ElderCare Locator – Connect with local Area Agencies on Aging
- Meals on Wheels America (1-888-998-6325)
- ABA Commission on Law and Aging – Legal resources and guardianship guidance
- Consumer Financial Protection Bureau – Managing Someone Else’s Money
- olderadultnestegg.com – resources for older adults, families, and professionals.
For Safety Concerns:
- National Center on Elder Abuse – Resources on recognizing and reporting abuse
- Report suspected abuse to Adult Protective Services (contact your local agency)
- Wandering: MedicAlert + Alzheimer’s Association Safe Return program (1-800-432-5378)
Download the Complete Guide: For a comprehensive reference, you can download the full handbook “Helping People Living Alone with Dementia Who Have No Known Support” which contains detailed strategies, case examples, and state-specific legal guidance.
A Personal Note
After decades of working with older adults facing cognitive challenges, I’ve learned that one of our greatest professional responsibilities is to see beyond the diagnosis to the person—their preferences, their history, their inherent dignity. Yes, dementia changes the brain, but it doesn’t erase personhood.
When someone is living alone with dementia, they’re not necessarily alone because they want to be or because no one cares. Sometimes they just haven’t been found yet. Sometimes the right supports haven’t been put in place. Sometimes a small intervention—a daily phone call, a medication organizer, a friendly neighbor checking in—makes all the difference between crisis and continued independence.
Our role is to be creative, persistent, and always—always—guided by respect for the individual’s autonomy and dignity. We work to enhance safety, not eliminate all risk. We provide support, not control. We honor choices while protecting wellbeing.
If you’re reading this because you’re worried about someone, please know that reaching out for help is not an overreaction. Early identification and intervention are infinitely easier than crisis management. Contact your local Area Agency on Aging, Adult Protective Services, or the Alzheimer’s Association helpline for guidance.
And if you’re a professional working with this population, thank you. This work requires patience, creativity, and heart. You’re making an immeasurable difference in the lives of some of our most vulnerable community members.
This blog post is based on the handbook “Helping People Living Alone with Dementia Who Have No Known Support” prepared by RTI International for the Administration for Community Living (September 2018). The full handbook contains extensive resources, legal guidance, and practical strategies for professionals working with this population.

Dr. Regina Koepp is a board certified clinical psychologist, clinical geropsychologist, and founder and CEO of the Center for Mental Health & Aging: the “go to” place for mental health and aging. Dr. Koepp is a sought after speaker on the topics of mental health and aging, caregiving, ageism, resilience, intimacy in the context of life altering Illness, and dementia and sexual expression. Dr. Koepp is on a mission to ensure mental health and belonging for older adults, because every person at every age is worthy of healing, transformation, and love. Learn more about Dr. Regina Koepp here.
Regina Koepp, PsyD, ABPP







































































Want More? Read Our Most Recent Posts


Older adults deserve high quality mental health care.
Therapists deserve the training to provide that care.
")