
Social Withdrawal or Healthy Social Selectivity?
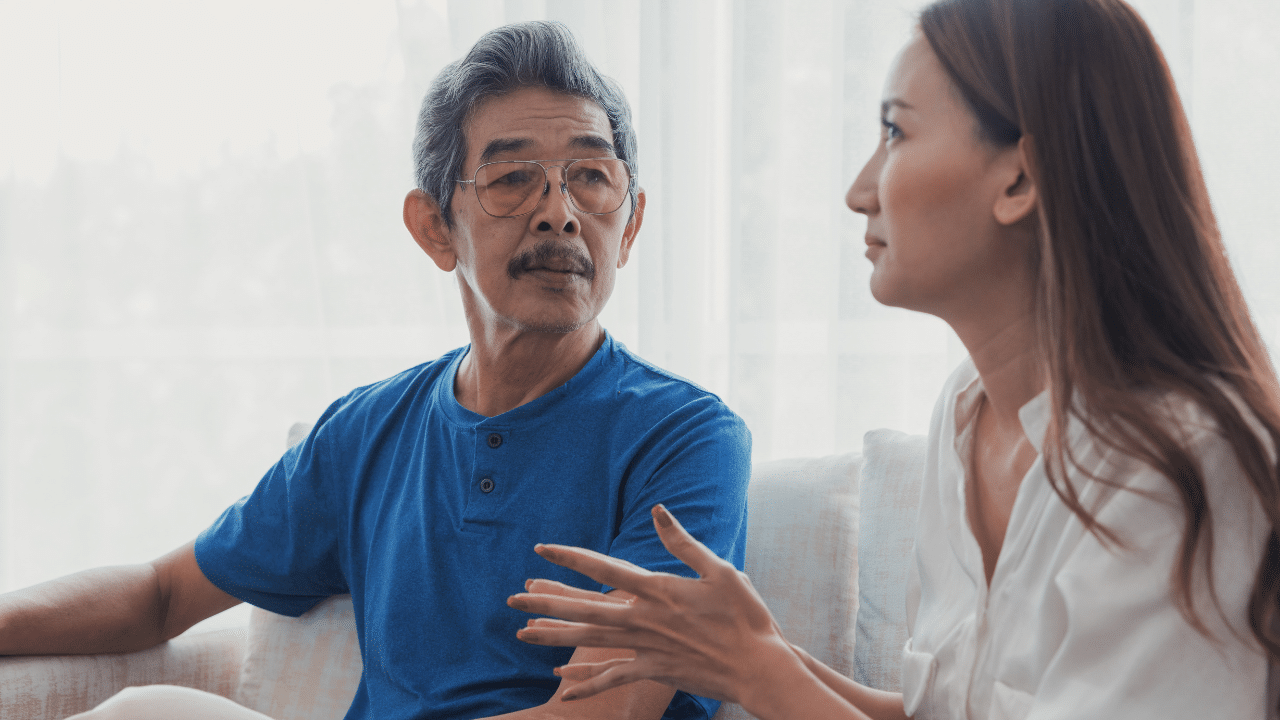
Your 83-year-old client’s daughter calls you concerned that her mother just quit her book club after three years and is concerned that her mom will now be isolated and lonely, what’s your first clinical hypothesis? Social withdrawal? Depression? Cognitive decline?
Before you take the daughter’s concern at face value, consider this: she may actually be just fine- maybe even better than fine.
“I didn’t quit connection,” she explains. “I quit small talk. Now I spend Wednesday afternoons having tea with my sister on Zoom, who lives 3,000 miles away. The conversation with my sister is what’s important to me.”
This is socioemotional selectivity theory (SST) in action. This theory can help us more accurately conceptualize healthy aging, set treatment goals, and distinguish adaptive pruning from clinical depression.
What Is Socioemotional Selectivity Theory?
Socioemotional selectivity theory, developed by Stanford psychologist Laura L. Carstensen, fundamentally reframes how we understand motivation across the lifespan. The central insight: our goals shift based on our perceived time horizon, not simply our chronological age.
When time feels expansive and open-ended (typically in younger adulthood), individuals tend to prioritize:
- Knowledge acquisition and skill building
- Novel experiences and exploration
- Expanding social networks
- Future-oriented preparation
- Information gathering, even when emotionally neutral or negative
When time feels limited or constrained (often in later life, but also after terminal diagnosis, major loss, or life transitions at any age), individuals tend to prioritize:
- Emotional meaning and present-moment satisfaction
- Deepening existing close relationships
- Value-aligned experiences
- Emotional regulation and positivity
- Legacy, coherence, and life integration
Research consistently demonstrates that older adults show enhanced emotion regulation, greater emotional complexity, and what researchers call the “positivity effect”—a tendency to attend to and remember positive information more than negative information (Carstensen & DeLiema, 2018; Mather & Carstensen, 2005).
Key Research Foundations
Carstensen’s seminal studies demonstrate that when younger adults are prompted to imagine limited time horizons (through experimental manipulation), they show preference patterns nearly identical to older adults—choosing familiar social partners over novel ones, prioritizing emotional meaning over information acquisition (Fung, Carstensen, & Lutz, 1999).
The theory has been validated across cultures, socioeconomic contexts, and clinical populations (Löckenhoff & Carstensen, 2004). Time perception—not age itself—is what motivates us.
How To Use Socioemotional Selectivity Theory Clinically: Pruning Relationships or Depression?
One of the most dangerous clinical errors with older adults is conflating intentional pruning with depressive withdrawal. Socio-Emotional Selectivity Theory gives us a framework to tell them apart.
The Fast Clinical Distinction
Adaptive Selectivity (SST-Consistent) may sound like:
- “I’m being more intentional about my energy.”
- “I want fewer relationships, but deeper ones.”
- “I realized that activity wasn’t adding anything meaningful anymore.”
- “I’m protecting what matters most to me.”
- Affect: Calm, clear, purposeful, sometimes relieved
- Function: Maintained or improved in priority domains
- Meaning: Preserved or enhanced
Depression may sound like:
- “Nothing feels worth it anymore.”
- “I don’t enjoy anything I used to love.”
- “I’m too much of a burden to reach out.”
- “Everything feels exhausting and pointless.”
- Affect: Flat, hopeless, guilty, heavy
- Function: Declining across domains, including valued ones
- Meaning: Collapsed, absent, or distorted (“I’m worthless”)
Assessment Questions
These questions may help you to get a quick impression
- “When you stepped back from [activity], what did that create space for?”
- Adaptive: Clear answer about meaningful alternative
- Depression: “Nothing” or “I just sleep more now”
- “Are you still doing things that feel important to you, or has everything felt less worthwhile?”
- Adaptive: Maintains valued activities
- Depression: Global anhedonia
- “Does this change feel like it’s in your control, or like something is happening to you?”
- Adaptive: Sense of agency
- Depression: Helplessness, passivity
- “On the relationships you’re keeping—are those feeling richer, or are you pulling back there too?”
- Adaptive: Deepening priority relationships
- Depression: Withdrawal from everyone, including closest connections
What to Do When The Person Experiences Both?
Sometimes you’ll encounter clients experiencing both depression and legitimate SST-driven selectivity. A client with moderate depression might still be making some adaptive social choices while simultaneously experiencing anhedonia in other domains.
Your treatment plan should address the depression while respecting and working with the selectivity where it’s values-aligned.
I walk through a vignette on how to do this in my upcoming CE course, Effective Therapy Therapy with Older Adults
Using SST to Build Rapid Rapport, Improve Clinical Assessment, and Make Your Treatment Aging-Informed
SST provides assessment questions that feel respectful, attuned, and clinically revealing—especially valuable with older adults who may be wary of therapists who don’t “get” their life stage.
Rapport-Building Questions Grounded in SST
Time Horizon Assessment:
- “When you think about the future right now, does it feel more open-ended, or more limited than it used to?”
- “Has anything changed recently that’s shifted how you think about time?”
Goal Orientation:
- “At this point in your life, what feels most important: expanding your options and trying new things, or deepening what already matters?”
- “When you imagine how you want to spend your energy in the next year, what comes to mind first?”
Social Selectivity:
- “Who are the 3 to 5 people you most want to invest your energy in right now?”
- “Have your social priorities shifted at all in recent years? If so, how?”
Values Clarification:
- “What makes this season of life feel important?
- “When you look at your typical week, which parts feel most meaningful?”
When a client feels truly understood at this level, therapeutic alliance is more likely to deepen—critical with older adults who may have limited treatment engagement history or skepticism about therapy’s relevance.
How To Use SST for Treatment Planning with Older Adults
SST isn’t an intervention—it’s a lens for identifying therapeutic goals and provides some helpful language to frame them.
When Time Feels Limited: Treatment Focus
For clients operating from a limited time horizon, treatment goals often work best when they emphasize:
- Emotional meaning and regulation rather than extensive skill-building for distant future scenarios
- Core relationship repair or deepening rather than expanding social networks
- Life review, legacy, and coherence work rather than future-oriented planning
- Present-moment quality of life rather than long-term prevention
SST-Aligned Therapeutic Interventions
- Life Review and Reminiscence Therapy: Structured life review helps clients construct coherent narratives, find meaning in difficult experiences, and achieve a sense of integrity over despair (Erikson’s final developmental stage). Evidence supports effectiveness for depression, life satisfaction, and preparation for end of life (Bohlmeijer et al., 2007).
- Meaning-Centered Psychotherapy: Adapted from Viktor Frankl’s logotherapy, meaning-centered approaches help clients identify sources of meaning (historical, attitudinal, creative, experiential) even in the face of loss and limitation (Breitbart et al., 2015).
- Relationship-Focused Interventions:
- Interpersonal Psychotherapy (IPT) adapted for older adults, often focusing on 1-2 key relationships
- Cognitive-behavioral approaches targeting relationship quality rather than quantity
- Dyadic interventions with spouses, adult children, or caregivers
- Values-Aligned Behavioral Activation: Rather than generic activity scheduling, identify 3-5 values and build activities explicitly around them: “What would make this week feel like it mattered?”
- Acceptance and Commitment Therapy (ACT): ACT’s emphasis on values clarification, psychological flexibility, and committed action aligns naturally with SST’s focus on meaning and selectivity (Skultety & Rodriguez, 2008).
When Time Feels More Open: Treatment Focus
When time horizon expands—perhaps following successful treatment, remission, or unexpected positive life transition—goals may shift toward:
- Skill development and learning
- Exploration and experimentation
- Expanding roles and identities
- Future planning and goal setting
- Broadening social connections aligned with new interests
Bottom Line: Match goals to time horizon, not to chronological age alone.
When Time Horizon Shifts Mid-Treatment
A client’s perceived sense of how much time they have left (also known as “time horizon”) isn’t static. It can shift rapidly, especially following:
- New medical diagnosis
- Bereavement
- Falls or functional decline
- Retirement or role loss
- Positive surprises (remission, new relationship, relocation to desired location)
- Societal events (pandemic, natural disaster)
When you sense a shift—goals that once resonated may now feel “off,” or suddenly the client’s priorities seem different—try this simple re-alignment question:
“How does time feel to you right now—more open and expansive, or more limited than it felt a few months ago?”
This single question often unlocks:
- Why previous treatment goals may no longer fit
- What the client actually needs now
- Permission to adjust the plan and recalibrate
Research shows that even within the same individual, a sense of how much time they have left can quickly change and as a result who they wish to spend time with as well as how they are making decisions may also quickly change (Fung et al., 1999).
It’s my belief that our work with our clients should be equally responsive.
Common Misapplications of SST (And How to Avoid Them)
Myth 1: “All older adults are in limited-time-horizon mode.”
Reality: Many older adults, particularly those who are healthy, recently retired, or beginning new chapters, experience time as quite expansive. A 73-year-old starting a second career or rekindling a romance may feel as if their time is expansive.
Clinical correction: Assess time perception individually. Don’t assume.
Myth 2: “SST means we should avoid challenging older clients or setting growth goals.”
Reality: SST helps you choose which growth goals will feel meaningful. Growth toward emotional depth, relationship repair, or legacy work may be far more motivating than growth in breadth or novelty.
Clinical correction: Reframe growth in meaning-centered terms when time feels limited.
Myth 3: “Selectivity is always healthy in older adults.”
Reality: Sometimes withdrawal is depression, trauma response, undiagnosed pain, caregiver burden, or internalized ageism (“I’m too old to do that”).
Clinical correction: Use the pruning vs. depression distinction framework above. Stay curious.
Practical Tools for Your Practice
The Social Energy Map (Values Exercise)
Ask clients to draw three concentric circles:
- Inner circle: People they want to invest the most emotional energy in
- Middle circle: People they want to maintain connection with, but less intensely
- Outer circle: People or activities they’re ready to release or minimize
Then ask: “What do you notice about the inner circle? What do those relationships have in common? What would nourish them?”
This exercise often reveals values and clarifies what “selectivity” is actually protecting.
The Meaning Audit (Treatment Planning Tool)
For clients in limited-time-horizon mode, try this values-clarification sequence:
- “What are 3-5 things that make life feel meaningful to you right now?”
- “How much of your typical week is spent on those things?”
- “What’s getting in the way of spending more time there?”
- “If we could shift that ratio even 10-15%, what would need to happen?”
The Clinical Bottom Line: Don’t Pathologize Pruning of Activities and Relationships —Assess Their Function
Older adulthood is not a slow fade into irrelevance. For many, it represents a profound and strategic shift toward emotional depth, meaning, and intentionality.
As clinicians, our role is not to push clients back toward busy-ness or productivity in ways that once defined earlier life stages. Or even Behavioral Activation for Behavioral Activation’s sake.
Our role is to help them:
- Invest energy where it creates genuine meaning
- Protect boundaries without withdrawing into isolation or loneliness
- Build a life that feels emotionally and spiritually meaningful —right now, in this body, in this season
Socioemotional selectivity theory gives us permission to honor that wisdom, rather than pathologize it.
When a client finally releases what no longer serves them to make space for what does, that’s not withdrawal. That’s clarity.
Want to Become an Aging-Informed Therapist?
Take one of our continuing education courses designed to help you meeting the mental health needs of older adults.
Remember, it’s only with your help that we can meet the mental health needs of older adults, so thank you for being here.
Want to Learn More About Socioemotional Selectivity Theory (SST)? Check out these resources.
Foundational SST Research:
- Carstensen, L. L. (2006). The influence of a sense of time on human development. Science, 312(5782), 1913-1915. https://doi.org/10.1126/science.1127488
- Carstensen, L. L., Isaacowitz, D. M., & Charles, S. T. (1999). Taking time seriously: A theory of socioemotional selectivity. American Psychologist, 54(3), 165-181. https://doi.org/10.1037/0003-066X.54.3.165
Clinical Applications:
- Knight, B.G., Poon, C.Y.M. Contextual Adult Life Span Theory for Adapting Psychotherapy with Older Adults. J Rat-Emo Cognitive-Behav Ther 26, 232–249 (2008). https://doi.org/10.1007/s10942-008-0084-7
- Segal, D. L., Qualls, S. H., & Smyer, M. A. (2018). Aging and Mental Health (3rd ed.). Wiley-Blackwell.
For exploring life review and meaning-centered approaches:
- Westerhof, G. J., Bohlmeijer, E. T., & Webster, J. D. (2010). Reminiscence and mental health: A review of recent progress in theory, research and interventions. Ageing & Society, 30(4), 697-721. https://doi.org/10.1017/S0144686X09990328

Dr. Regina Koepp is a board certified clinical psychologist, clinical geropsychologist, and founder and CEO of the Center for Mental Health & Aging: the “go to” place for mental health and aging. Dr. Koepp is a sought after speaker on the topics of mental health and aging, caregiving, ageism, resilience, intimacy in the context of life altering Illness, and dementia and sexual expression. Dr. Koepp is on a mission to ensure mental health and belonging for older adults, because every person at every age is worthy of healing, transformation, and love. Learn more about Dr. Regina Koepp here.
Regina Koepp, PsyD, ABPP







































































Want More? Read Our Most Recent Posts


Older adults deserve high quality mental health care.
Therapists deserve the training to provide that care.
")