
A clinician in my Mental Health + Aging Certificate program recently asked a question. He was reflecting on the opening module — the one where I lay the foundation for who we are providing therapy for, where I explore intersecting identities, share important statistics, and name the harm created by queerphobia, racism, classism, and other forms of systemic oppression.
Here’s what he said: “I’m concerned about the emphasis on LGBTQ+. Why? Only 4–5% of the elderly identify as such. I’m just not getting it.”
I appreciated the question. It told me he was thinking critically about how we allocate learning time, and that’s exactly the kind of reflection good training should cultivate.
His assumption deserved a direct response, because it’s one I hear regularly — and it rests on a fundamental misunderstanding of how equity-centered education works.
We don’t allocate training time based on population size. We allocate it based on need, historical harm, and the gap between what providers know and what their clients require. LGBTQ+ older adults sit at the intersection of all three.
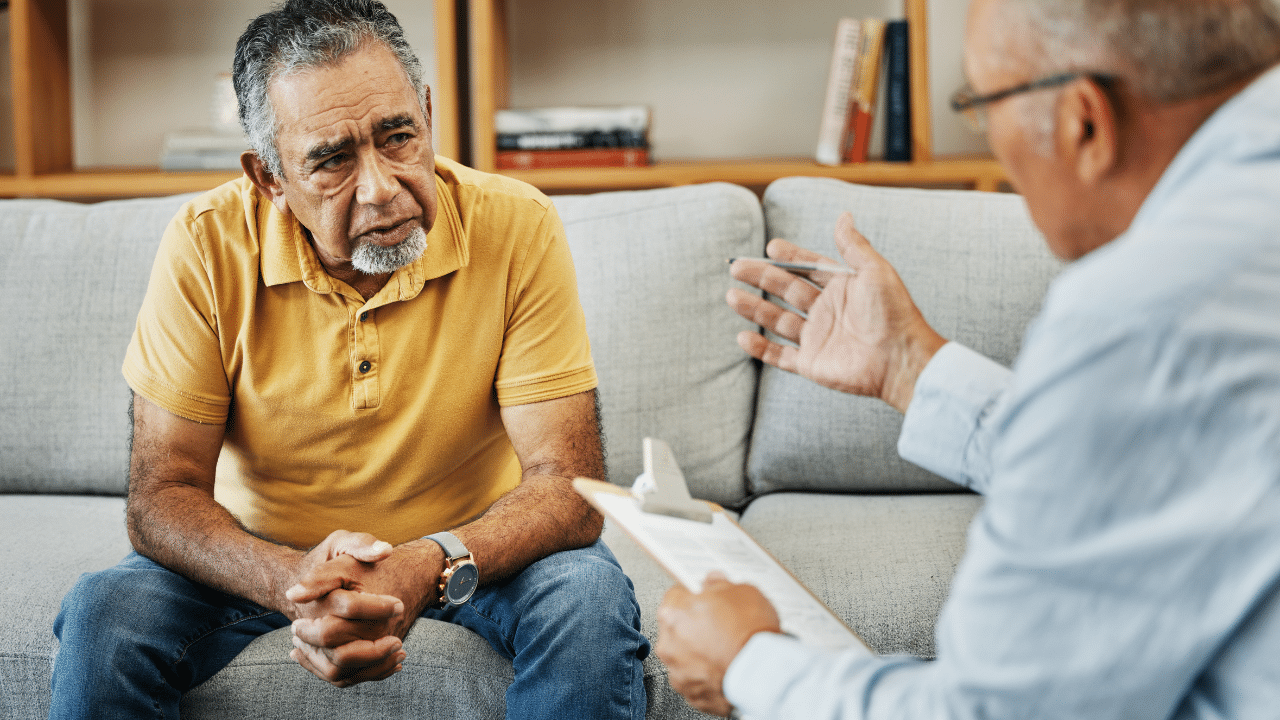
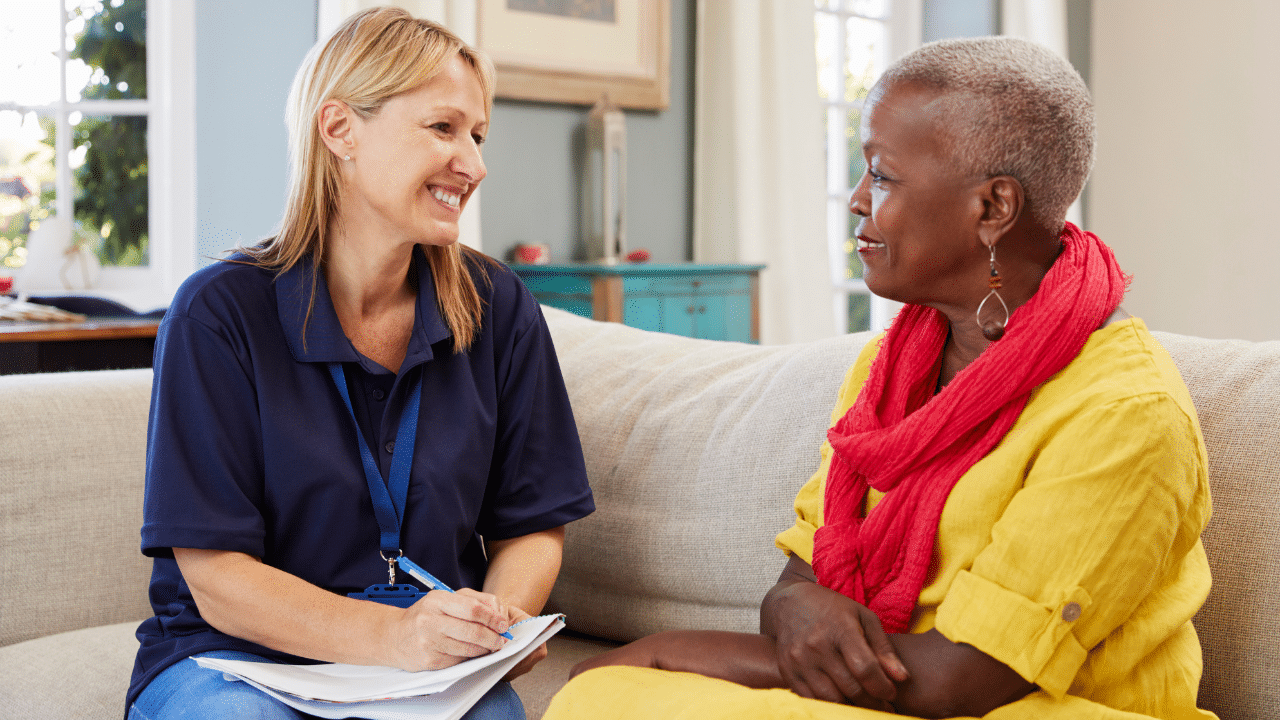
Once, in the span of six weeks, two older men — both married to women, each working with me in individual psychotherapy to manage depression and anxiety — revealed that they’d had same-sex relationships earlier in their lives. While they loved their spouses, they feared their lives would end without ever experiencing that kind of deeper love again. We spent several sessions processing the suffering that LGBTQ-phobia had caused them, grieving the missed opportunities, and creating a space where they could be seen and valued for who they are.
As therapists, it’s on us to help repair some of the damage that has been done to our LGBTQ+ clients excluded from communities, relationships, and love — then and now.
Neither of those clients would have disclosed if I hadn’t created the conditions that made it possible. And they wouldn’t have disclosed at all if I had assumed, because they were older and married to opposite-sex partners, that their sexual history and identity were settled questions.
Don’t assume your older client’s straight.
Ageism, Queerphobia and the Damage of Invisibility
Helping clinicians I train and consult with discover just how harmful ageist thinking is can feel like a significant undertaking.
Now layer LGBTQ+ identity onto that. The intersection of ageism and queerphobia compounds the harm. Studies show that many LGBTQ+ older adults fear having to re-closet themselves when moving into a long-term care community — and that when the time comes, many do choose to hide their sexual orientation for their own safety and security in a new community.
The experience of transgender older adults is even more stark: studies have found that some older transgender individuals report preferring death to moving into a long-term care setting (Fredriksen-Goldsen et al., 2013). That is the weight of a life lived under relentless harm. It’s a clinical reality we are obligated to understand.
Our Field Caused Harm — and We Have a Professional Obligation to Address It
Many of today’s LGBTQ+ older adults came of age during the McCarthy era, a period of active government persecution of gay and lesbian individuals. Same-sex relationships were classified as pathological in the DSM until 1973 — well within the lifetimes of many clients sitting in our offices today.
Our field caused harm. Providing focused clinical education is one direct, concrete way to repair that legacy and ensure we’re not still contributing to it.
The Mental Health Burden LGBTQ+ Older Adults Carry Into Your Office
Depression. Anxiety. Loneliness. Suicidality. These aren’t just elevated risks for LGBTQ+ older adults — they show up across the research consistently, across populations, across decades.
Among a national sample of LGBT older adults, nearly one-third screened positive for depression — significantly higher than their heterosexual peers (Fredriksen-Goldsen et al., 2013). A large population-based study using 2023 Behavioral Risk Factor Surveillance System data found that LGBT+ older adults report greater rates of depression (22% vs. 15%), are nearly one-third more likely to experience loneliness than non-LGBT+ older adults, and are disproportionately more likely to be unmarried or unpartnered (61% vs. 46%), to have lower incomes, and to face food and housing insecurity (Flatt et al., 2025). These aren’t marginal differences. They are consistent, measurable, and clinically significant.
A 2025 longitudinal study from the Canadian Longitudinal Study on Aging examined mental health trajectories over time in LGB and heterosexual midlife and older adults. LGB adults reported significantly higher psychological distress and depression symptoms, and lower life satisfaction, across the study period. Bisexual adults showed particularly persistent disparities that did not resolve with age. The authors concluded that cumulative minority stress — not identity itself — drives these outcomes (Courtice et al., 2025).
Suicidality follows the same pattern. A landmark study published in American Psychologist examined mortality risk in over 834,000 middle-aged and older adult Veterans — including 167,676 who identified as LGBT — using VA healthcare data from 2009 to 2019. In initial analyses, LGBT Veterans had significantly higher rates of death by suicide and overdose compared to non-LGBT Veterans. Researchers looked deeper and found that elevated risk isn’t something inherent to being LGBTQ+. It is the accumulation of minority stress, stigma, and unaddressed health vulnerabilities across a lifetime (Beaudreau et al., 2026). Intervene on those factors, and you can change outcomes. That is a clinical mandate.
The isolating effects of a lifetime spent concealing identity compound all of this. LGBT older adults are less likely to be married or partnered, more likely to be estranged from families of origin, and approximately 55% report living alone — making their naturally occurring support networks smaller and less available precisely when people need them most (Fredriksen-Goldsen et al., 2013).
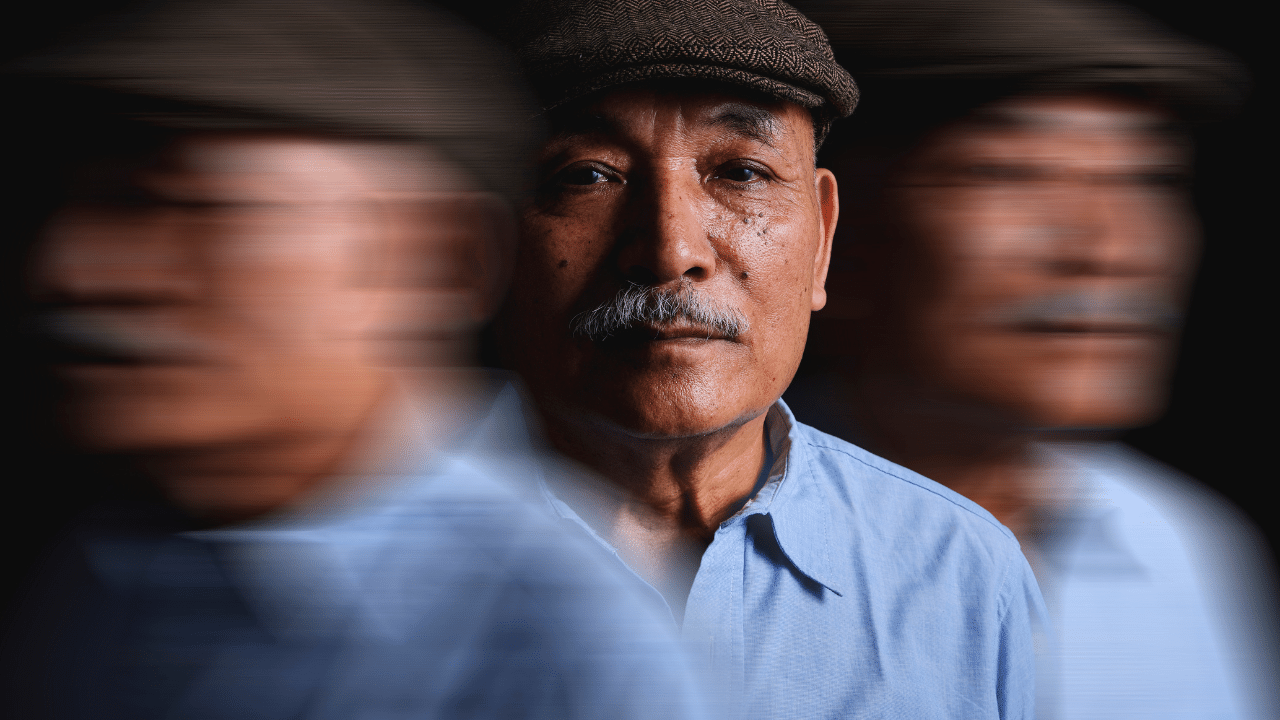
A client’s grief, withdrawal, or anxiety may have roots you’ll never see if you’re not trained to look.
A client presenting with depression may be grieving a partner they were never legally able to marry. A client who seems withdrawn may have spent sixty years calculating whether any given room was safe enough to be themselves in. A client’s anxiety may be rooted not in current circumstances, but in a lifetime of learning that who they are requires protection.
You won’t see any of that if you’re not trained to look for it.
The “4–5%” Statistic Significantly Undercounts This Population
Yes, approximately 4–5% of older adults openly identify as LGBTQ+. But recent Gallup polling shows that roughly 20% of Gen Z self-identifies as LGBTQ+ (Gallup, 2024). The lower rates among older cohorts don’t reflect a smaller population — they reflect the profound impact of living through criminalization and medicalized shame.
Many older adults in same-sex relationships, or with same-sex histories, will never disclose on a census form or an intake questionnaire. They have learned, over decades, that disclosure is not safe. They will, however, sit across from you in a therapy room. You need to know how to hold that with clinical skill and without assumption.
Equity in Training Means Proportionate Response to Need — Not Equal Distribution of Time
If a subgroup is more likely to be harmed by undertrained providers, they deserve more focused attention in a clinical curriculum — not less. This is the same logic that drives how we teach dementia care.
Only about 1 in 10 people over 65 has dementia. Yet in our mental health and aging programs, we spend significant time on it — because the stakes of getting it wrong are high and the training gap is real. The same is true here.
Equity in education isn’t about giving every group an equal slice of time. It’s about asking: where is the gap between what clinicians know and what their clients need? And then closing it.
The question isn’t ‘how many of my clients identify this way?’ It’s ‘am I clinically prepared for the ones who do?’
What This Means for Your Practice
You may already be seeing LGBTQ+ older adults in your practice and not knowing it. You may be asking intake questions that inadvertently signal that disclosure isn’t safe. You may be missing grief that looks like depression, or social isolation that stems from family rejection decades ago.
The goal of including LGBTQ+ older adults in our training programs isn’t to check a box. It’s to make you a more thoughtful, inclusive, and ethical clinician — one who sees the full person sitting in front of you. That’s what the mental health and aging field requires of us.
So, instead of asking “Why focus on LGBTQ+ older adults?” consider asking:
- “What can this teach me about how I look at the world and the person sitting in front of me?”
- “How do I hold a universal experience — one of growing older — alongside a person’s unique experience at the same time?”
- “How am I showing up for my clients in a way that honors who they are?”
And, for the brave among us:
- “How might I be contributing to the minority stress my clients already carry — the stress that makes them more vulnerable to physical illness, depression, and early death? And what am I willing to do differently?”
These are not comfortable questions. They’re the right ones.
If these are the kinds of questions that you’re open to asking, then you’ll love our mental health and aging training programs.
Systemic oppression causes real, measurable harm. It also has a remedy. It starts with you.

Dr. Regina Koepp is a board certified clinical psychologist, clinical geropsychologist, and founder and CEO of the Center for Mental Health & Aging: the “go to” place for mental health and aging. Dr. Koepp is a sought after speaker on the topics of mental health and aging, caregiving, ageism, resilience, intimacy in the context of life altering Illness, and dementia and sexual expression. Dr. Koepp is on a mission to ensure mental health and belonging for older adults, because every person at every age is worthy of healing, transformation, and love. Learn more about Dr. Regina Koepp here.
Regina Koepp, PsyD, ABPP







































































Want More? Read Our Most Recent Posts


Older adults deserve high quality mental health care.
Therapists deserve the training to provide that care.
")